Cannot be more grateful that’s done! (FM1/IM1)
And in the blink of an eye, FM1/IM1 is over!
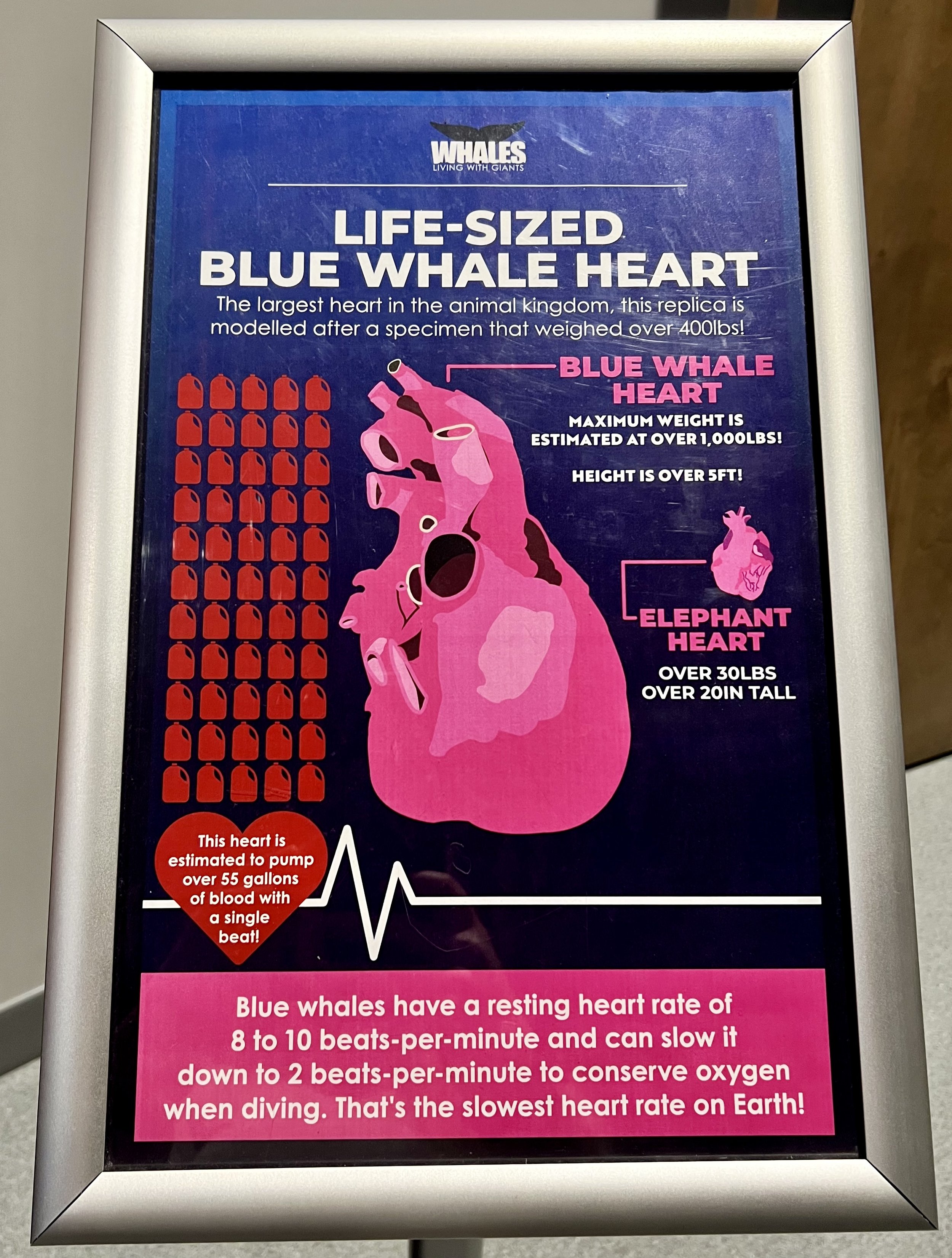

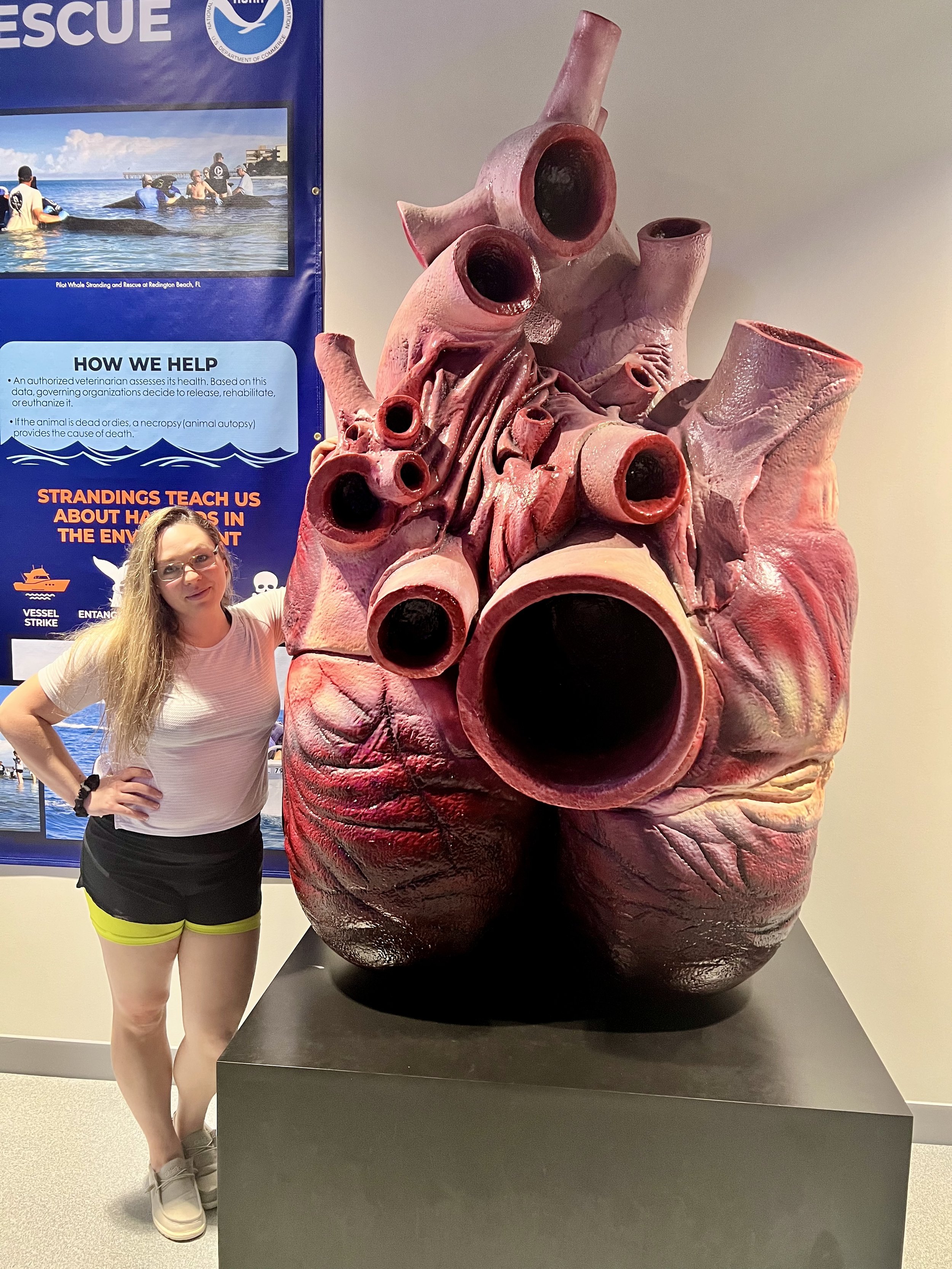
Okay, so these pictures aren’t exactly from my rotations, but (IYKYK), my passion is cardiology, and when I saw this (ACTUAL SIZE) replica of a Blue Whale heart from Clearwater Marine Aquarium in Clearwater, Florida, I just HAD to include it in this post!
My overall thoughts….
I’ve had some time to process my experience during FM1/IM1 in Ohio and I must say, I echo the sentiments expressed in my first blog post about this rotation (if you haven’t read that one, click here!)
I spent 2 weeks in the Emergency Department, 2 weeks in a Family Medicine rotation, 2 weeks in Internal Medicine, and 2 weeks in Urgent Care (although the final week was more for didactics and final presentations). I wish I had more pictures to show you, and I promise I’ll work on that, but it’s difficult when you’re first trying to find your footing and seeing exactly what the boundaries are. You also have to prepare a student portfolio that includes patients you saw, procedures you observed or performed, presentations you did, and academic activities you took part in. The last part of the portfolio included three case studies which I based them off of H&Ps I had to submit to the coordinator. Finally there was an OSCE that final week. This is the standard curriculum that doesn’t include anything your residents have you do. I had to do some research into various diagnoses a few times and present those findings with the attending and/or resident.
I’ll break down each of these rotations below and my thoughts and what I got to do, but I just want to say that I loved the structure of the program. I honestly felt like this was a great way to introduce clinical medicine. I was able to ask questions without feeling judged, I was allowed to not know things, I was allowed to explore my own routine for completing a patient interview. It was a low stress way to get used to the idea of our roles as medical students in a clinical setting. Now, I know this joy and appreciation might not be there for each rotation, but as a way to start off third year, I don’t think I could have asked for a better experience.
The attending physicians and residents are approachable and patient. The coordinators are really great at communicating and making you feel comfortable. The program has lots of activities built in to make sure you are always learning something, even on easy days. But, I do want to say, I chose to have a very active role in my education. I chose to ask questions and be curious and try to be as hands on as possible. If you want to skate by and do the bare minimum, I do feel like you could get away with that. I would challenge you, however, that you are in this field to help others and to do that, you need to be curious and you should want to gain as much skill as you can when you have the opportunity. I know it may feel awkward or you may have difficulty speaking up, but this first elective is an amazing way to get used to doing just that. There are no expectations set for you, so you need to set the expectation yourself.
By the way, these things are a MUST for rotations, I used these so much and they were so helpful! I wasn’t the only one either, a bunch of people out of my 15 people cohort used these exact same things. (Amazon affiliate links)
Bifold Clipboard that fits Med Basics Notebook
Trifold Clipboard (for smaller pockets)
Awesome Pens that don’t click loud and write smooth
Any suture practice bundle, I use this one.
Weeks 1-2 Emergency Department
During my time in the ED, I learned how to access the computer and patient information on MediTech, which is the EMR this hospital uses. It took some trial and error as we were left to figure that out on our own, but we got there in the end! Having access to the records really helped in writing our H&Ps so we could see the full history or our patients and also what room number they were in. I would say mostly for the first week I shadowed the attending, but I eventually worked up the courage to ask to see patients. I would go see the patient first, do the initial interview and physical exam which was all focused on their complaint, and report this back to the attending. He would then go with me to see the patient again and I would get to see what questions I missed or forgot to ask and if I performed something in the physical exam wrong, he would correct that. It also allowed us to talk about possible differentials and treatments.
Antibiotics are probably the most prescribed and the hardest to learn in the clinical setting. The physicians usually use brand names at this point so there was a lot of googling I had to do lol. It also turns out that antibiotics are cycled based on the ones that are most resistant during that specific period of time, so while you may be giving out levofloxacin a lot for this month, next month that may have high resistance and you may be giving the patients a different antibiotic. All this to say, don’t get frustrated with yourself if there are things you still don’t know. You really start to realize how much more there is to learn, and It’s a lot and overwhelming lol, but we are taking things one step at a time!

I also got to see some really cool procedures, like this one on the right called Fluorescein eye stain which helps to visualize a corneal abrasion or other debris in the eye. I also got to assist with inserting staples to close a laceration on the head. I watched a chest tube insertion and also assisted with CPR. Finally, I learned how to use an otoscope and exactly what I’m supposed to be looking for during ear exams. The ED was the most hands on I think, but I also was able to see quite a few interesting patients and learn a lot from them. It was also the most fast paced, so it was really important to try and keep up and there were times where it was not time to learn, but just pitch in wherever you could. This was my favorite of the whole program.
Weeks 3-4 Family Medicine
Family Medicine is not for me haha. I realized that pretty quickly during this rotation, but it is necessary and part of the core requirements so I tried to make the best of it. It is a difficult rotation because you have to know so much of everything: geriatrics, pediatrics, minor trauma care, orthopedics, OB/GYN, general medicine, etc. That also means that come time for the actual core and shelf exam, they say this is the toughest. So I have already started prepping for this shelf exam even though I don’t begin my Family Medicine rotation until the end of January. There is only 6 weeks to try and learn everything, and that timeline feels so short!
The only interesting thing I really have to report here is that we learned how to do IUD insertions during our didactics session. While in FM, you have to do didactics which is basically group learning every Wednesday, and on one of those days a company was brought in that showed us how to do the IUD insertion and that was really cool to learn and see (and realize how painful it is!) Most of this rotation involved very quick visits with patients, most of them were not acute cases but follow ups regarding existing problems. It was a good experience to learn what FM entails and the unique needs of our patients here. However, it is a bit slow paced for me personally. I can see how others may enjoy the rigid learning required to be a super competent FM physician though, and if you want to be a physician that really connects with their patients and gets to care for them and their families for years, this would be an awesome speciality for you! There are definitely great things about this area of medicine, but first impression, not really my cup of tea.
P.S. I was told to use this FM Case Files book for shelf prep and that it was a life saver.
Weeks 5-6 Internal Medicine
Internal Med is similar to family med, except you are in more of a hospital setting and treating chronic illnesses during acute patient visits. There is also a lot of knowledge required to do internal medicine but it’s a great bridge to other specialities like cardiology or pulmonology. This rotation took up the most amount of time. You had to report to the hospital by 6:30 am and were there until 1 pm at the earliest, sometimes you didn’t leave until 3 or 4. It really depends on the resident you are following and how long it takes to get through patient rounds. When you arrive in the morning, you meet with your resident and usually get assigned a patient, but it depends what resident you have. Some residents want you to round with them on all their patients, others prefer you only take one patient. I had both experiences since I worked with two different residents. Once you get assigned a patient or patients, you look them up in the EMR and start researching why they were admitted and any acute changes they are having. You go and see your patient and complete your assessment and plan for them. This was the first time I actually got to write in the EMR! My resident showed me how to do a medical student progress note and I was able to complete a full note for a patient and she critiqued it. She also showed me how to write a good SOAP note and what she usually includes in hers.
There was SO much I learned during this rotation. While the ED was the most hands-on, this one was the most in terms of acquiring knowledge. I had a lot of research to do and report back to the residents. I presented a few cases to the attending physician during rounds, and I was honestly treated like an actual core student or resident during this time. It was an incredible experience. Even though the hours were long, I enjoyed this rotation a lot. It takes a lot of work to be an internist, that’s for sure, and you feel dumb quite a lot lol, but it is so worth it to start to gain so much knowledge. I could talk for DAYS about all that I learned here but suffice it to say that this rotation will challenge you, intrigue you, and humble you all at once!
P.S.S. I bought these IM books recommended by my clinical mentor and they have been of amazing use already!! (They are heavy and the paper is so thin omg, but the information is perfection.
Weeks 7-8 Urgent Care and Final Presentation
Ah, Urgent Care. Yes. It was an experience. Not a bad one, just that EVERY PATIENT HAD AN UPPER RESPIRATORY INFECTION. I am not kidding lol. I know how to treat a URI very well now lol. The attending physician we had during this rotation was awesome. He didn’t even seem like he was an attending because his attitude towards us was so friendly and engaging. He treated us as equals and not to say that this doesn’t happen, but usually you can feel the power structure set by this field. He was interactive, knowledgable, and cared to give us solid advice and direction. Most days we were excused early because there just weren’t a lot of patients, but we still made the best of the patients we did have. I will say, seeing strep throat in person for the first time is something you won’t forget once you’ve seen it! Not much else to report here, although the location of the urgent care was about a 20-25 minute drive from the hospital so that is something to note.
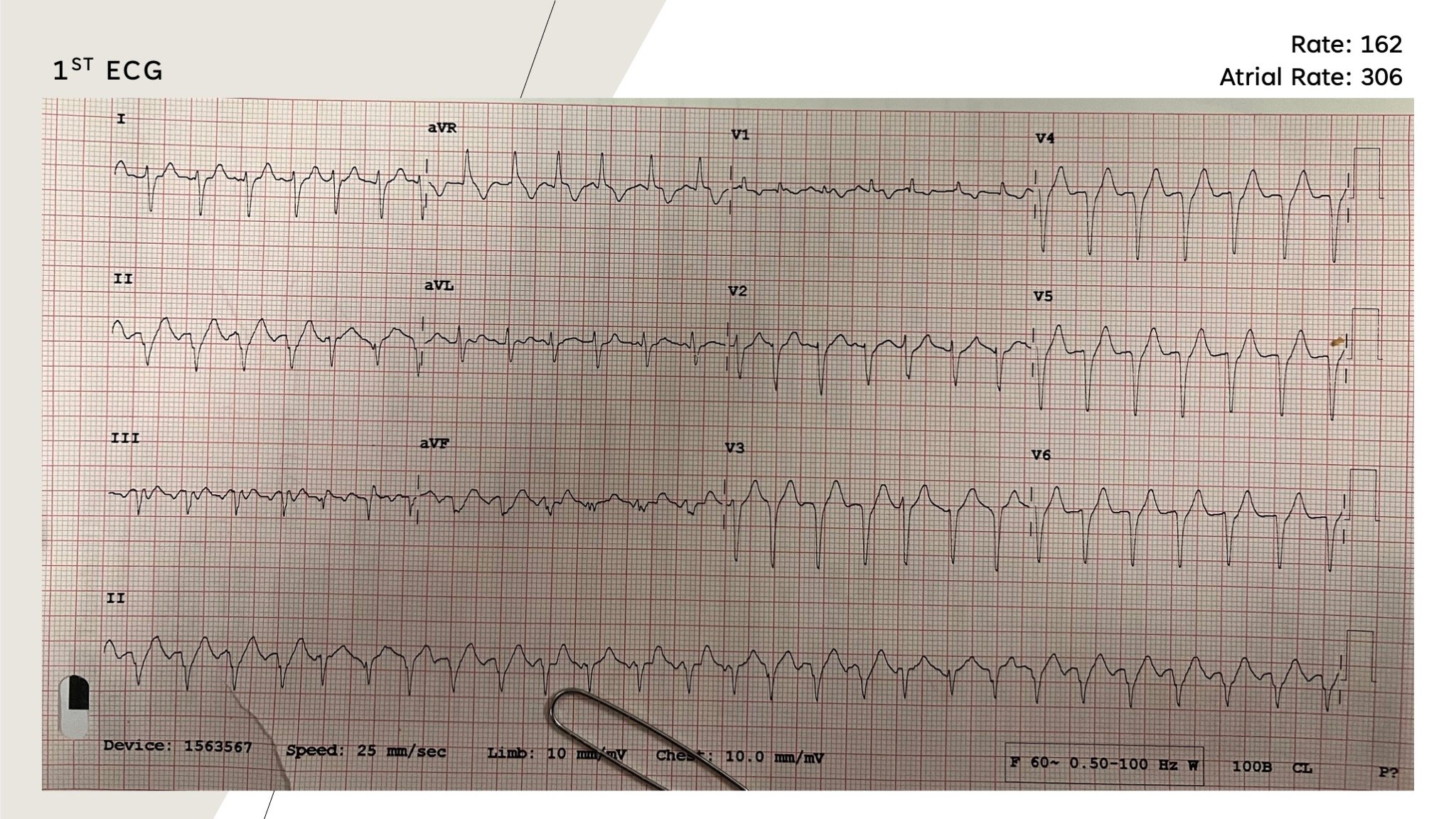
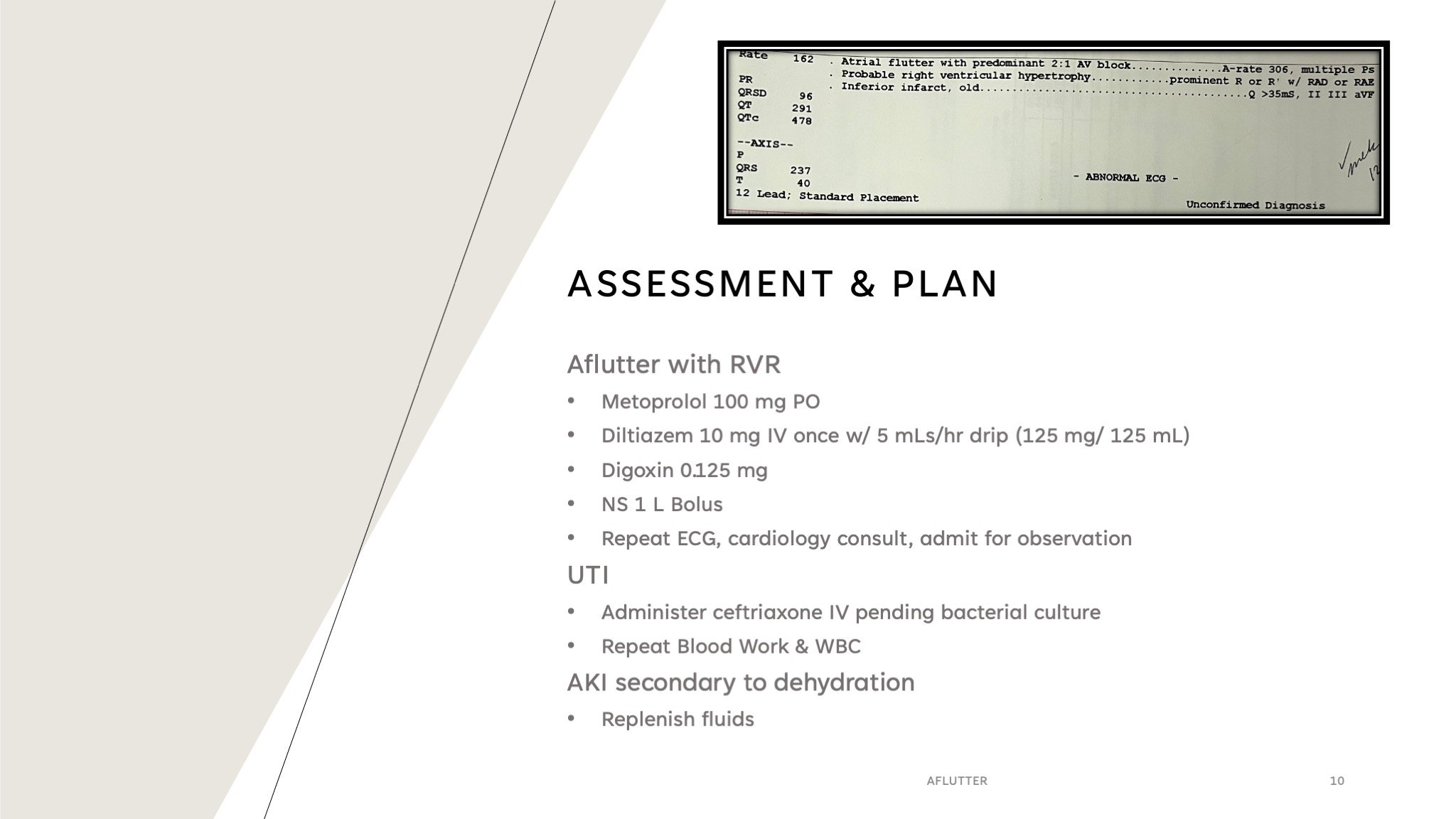
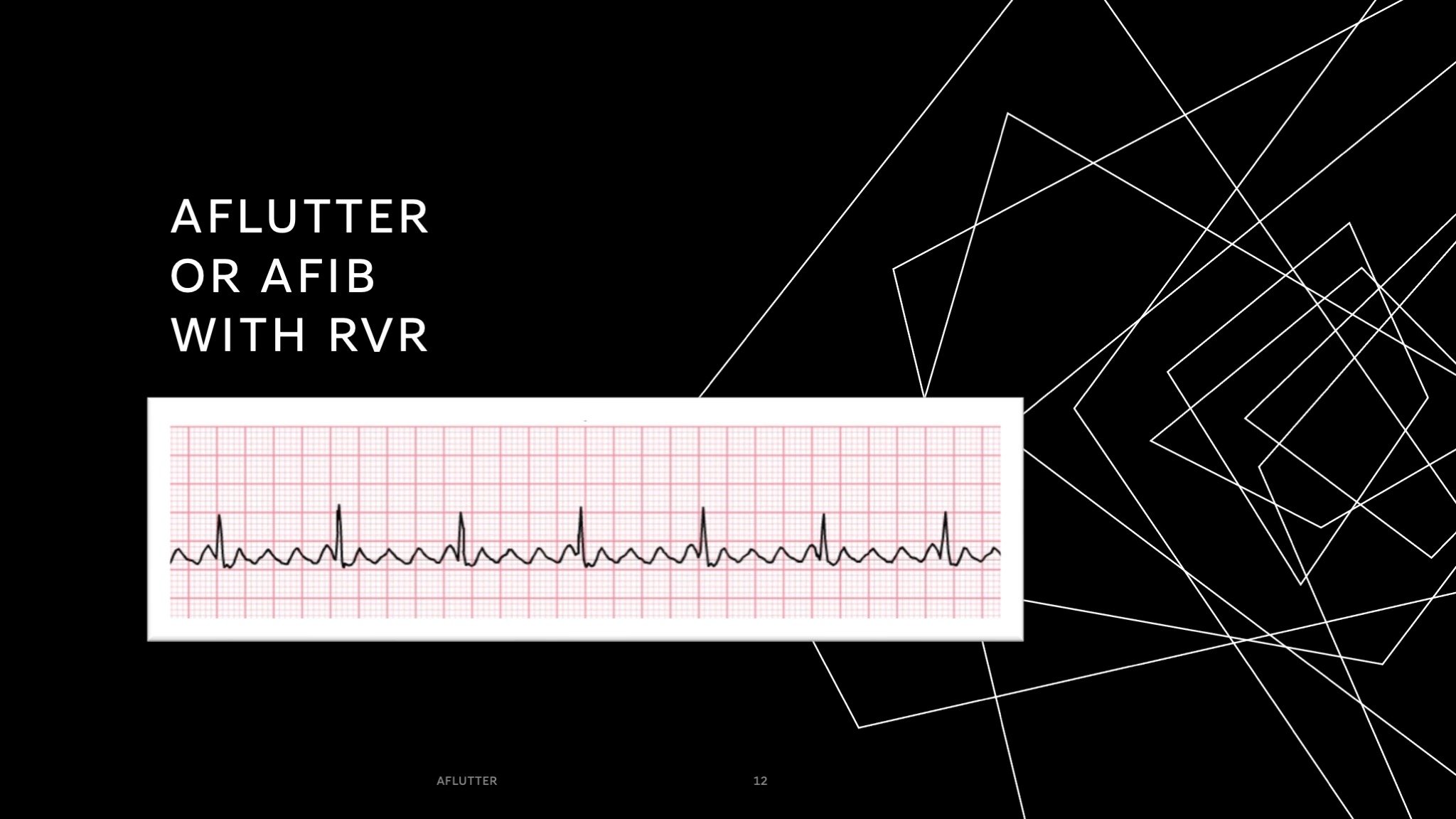
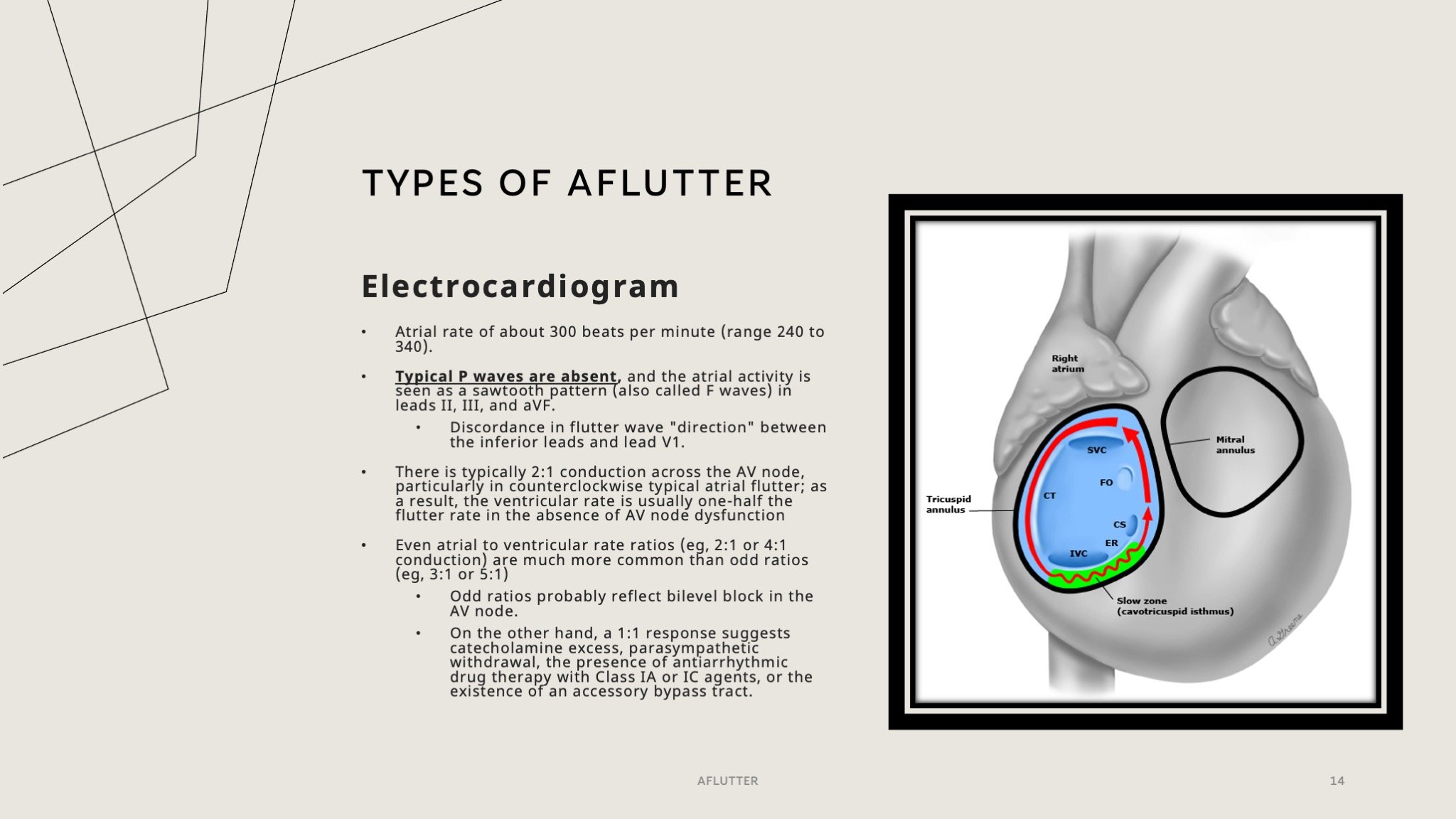
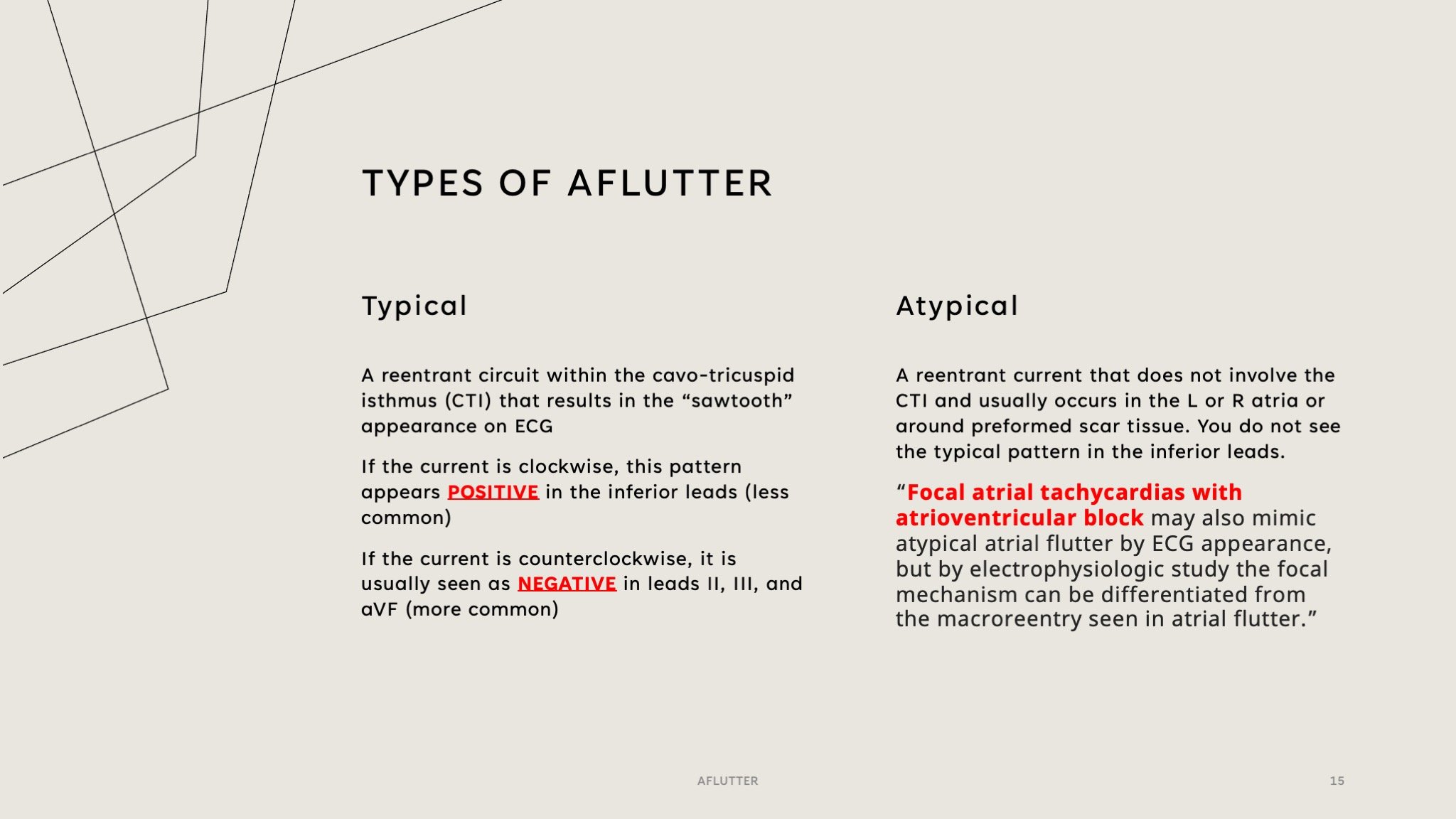
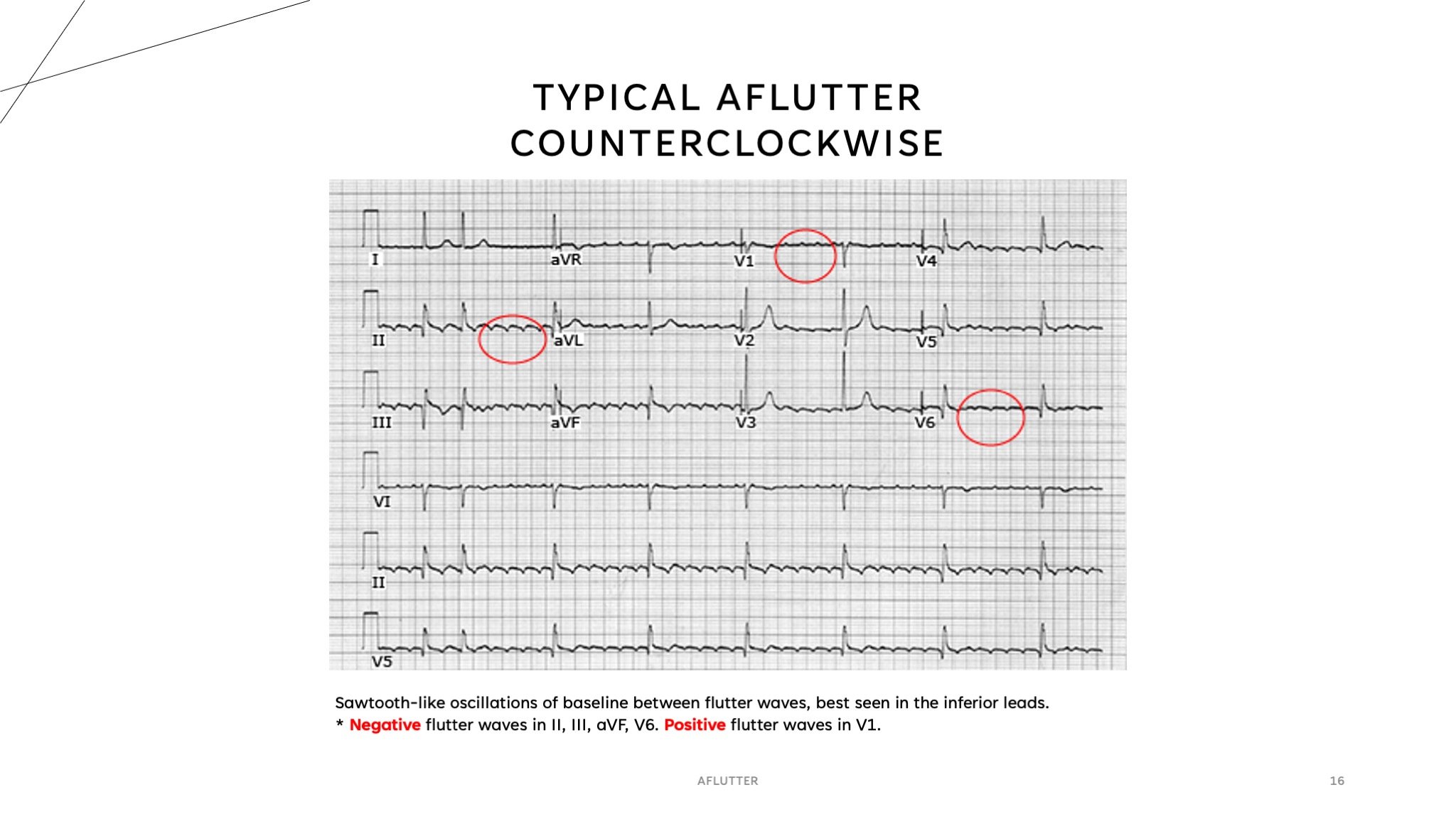
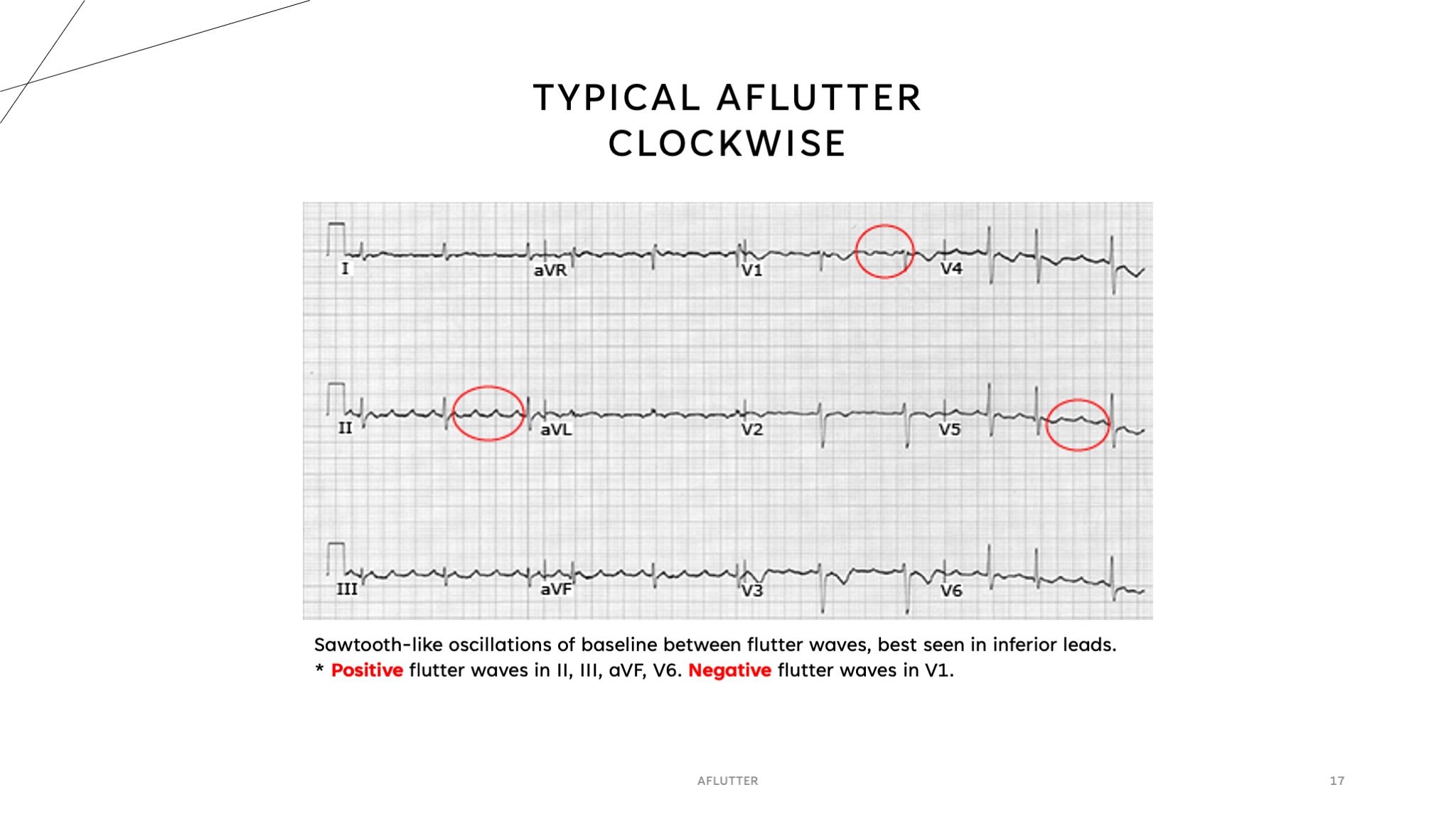
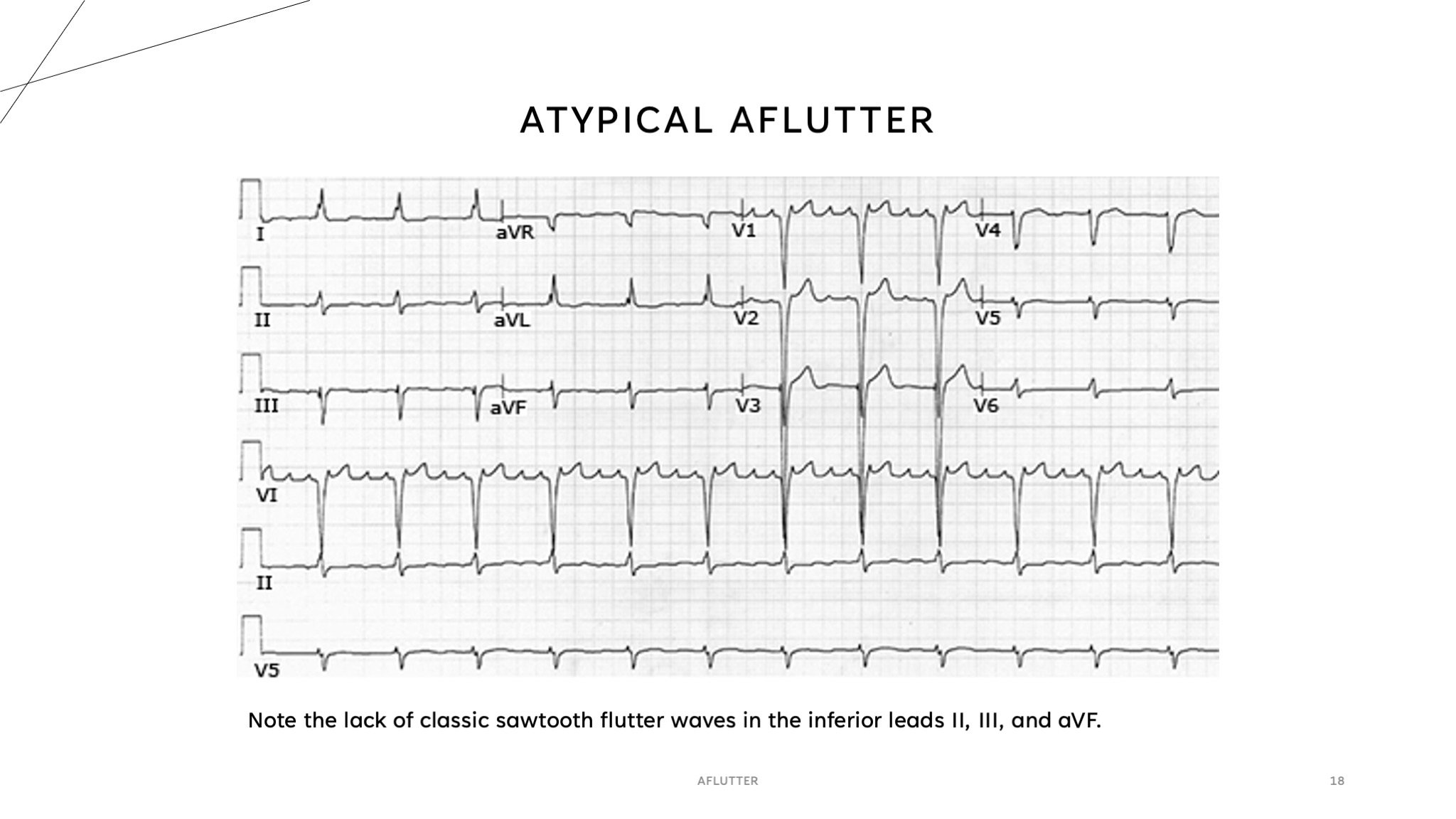
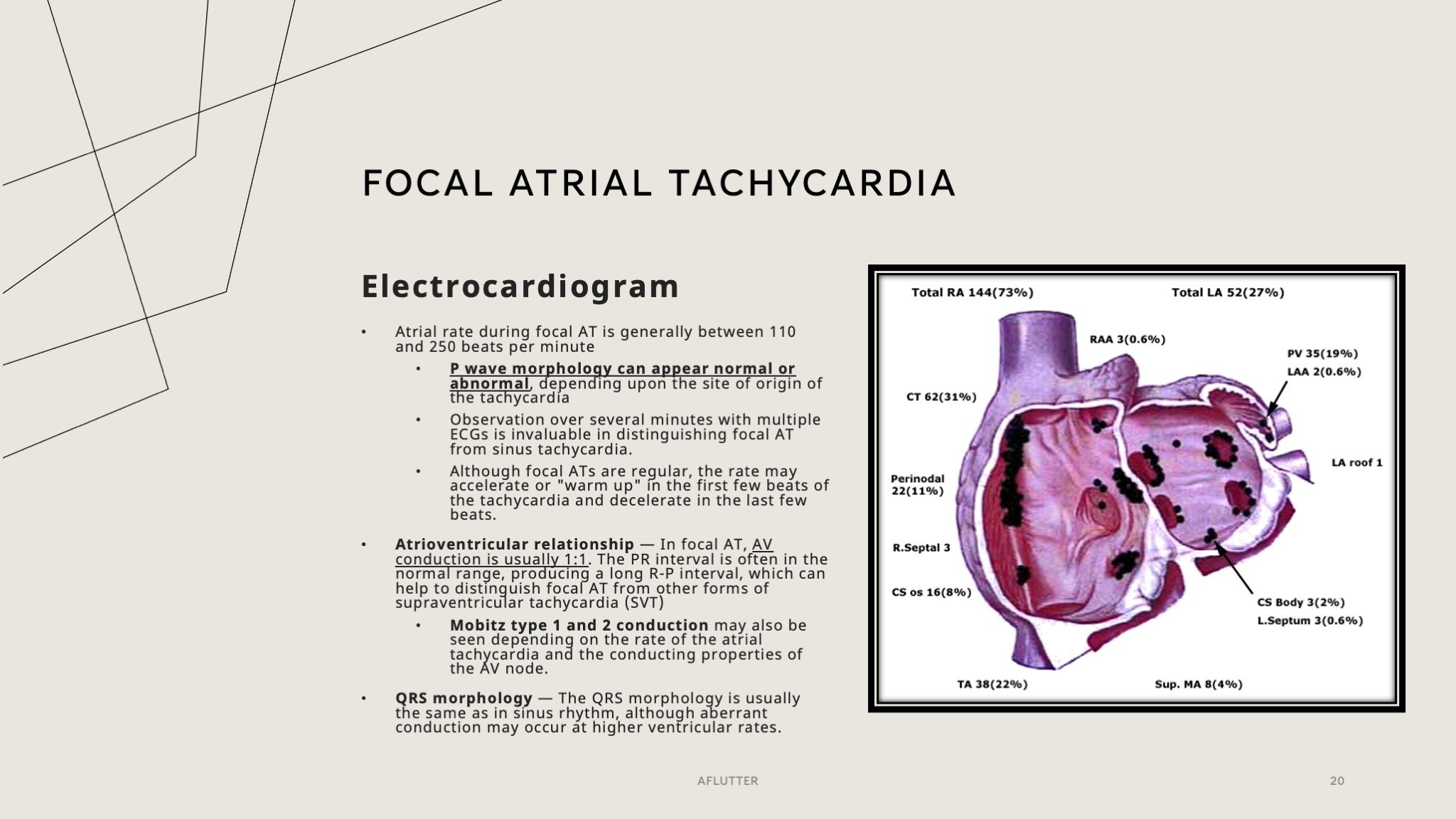
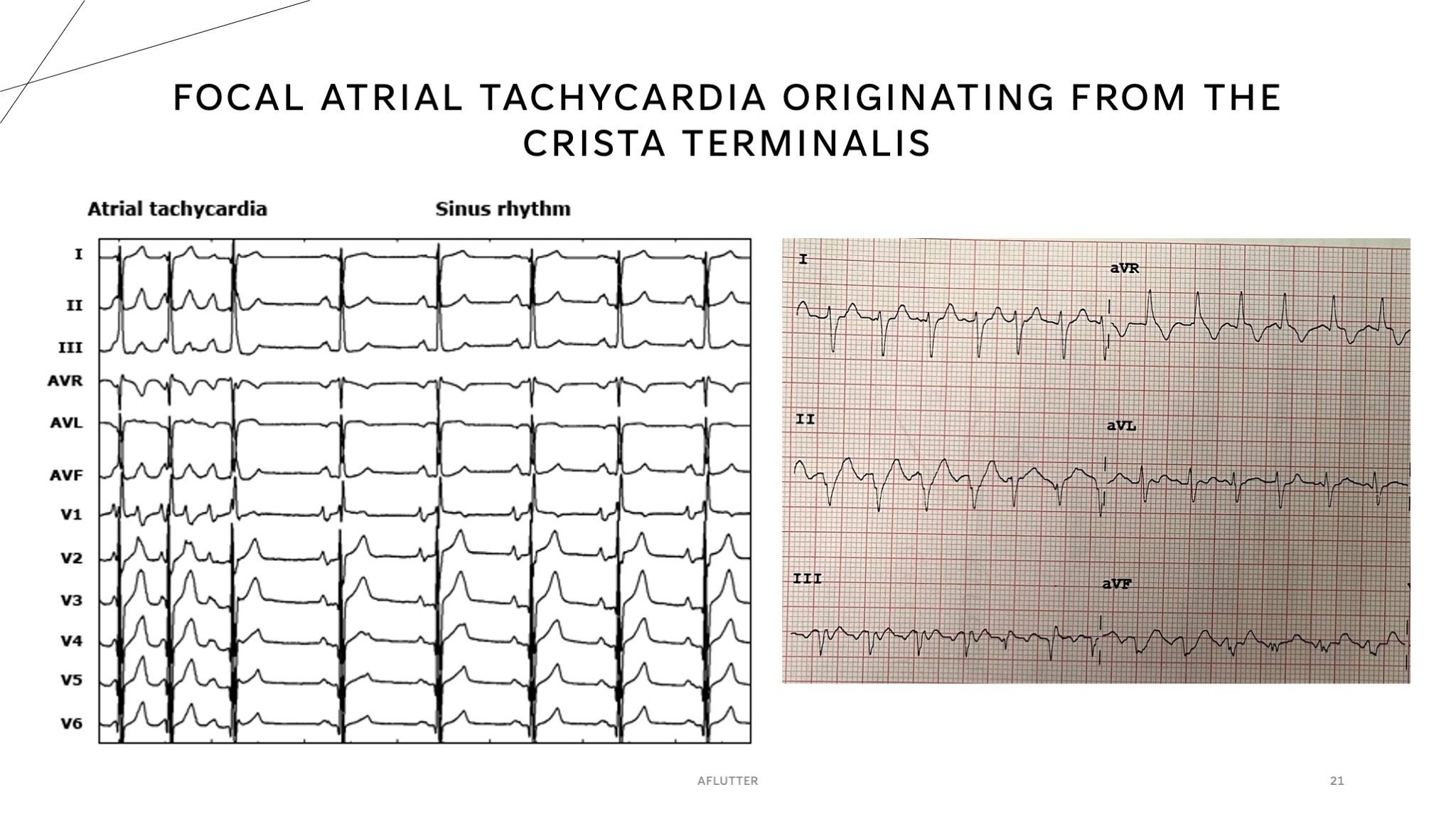
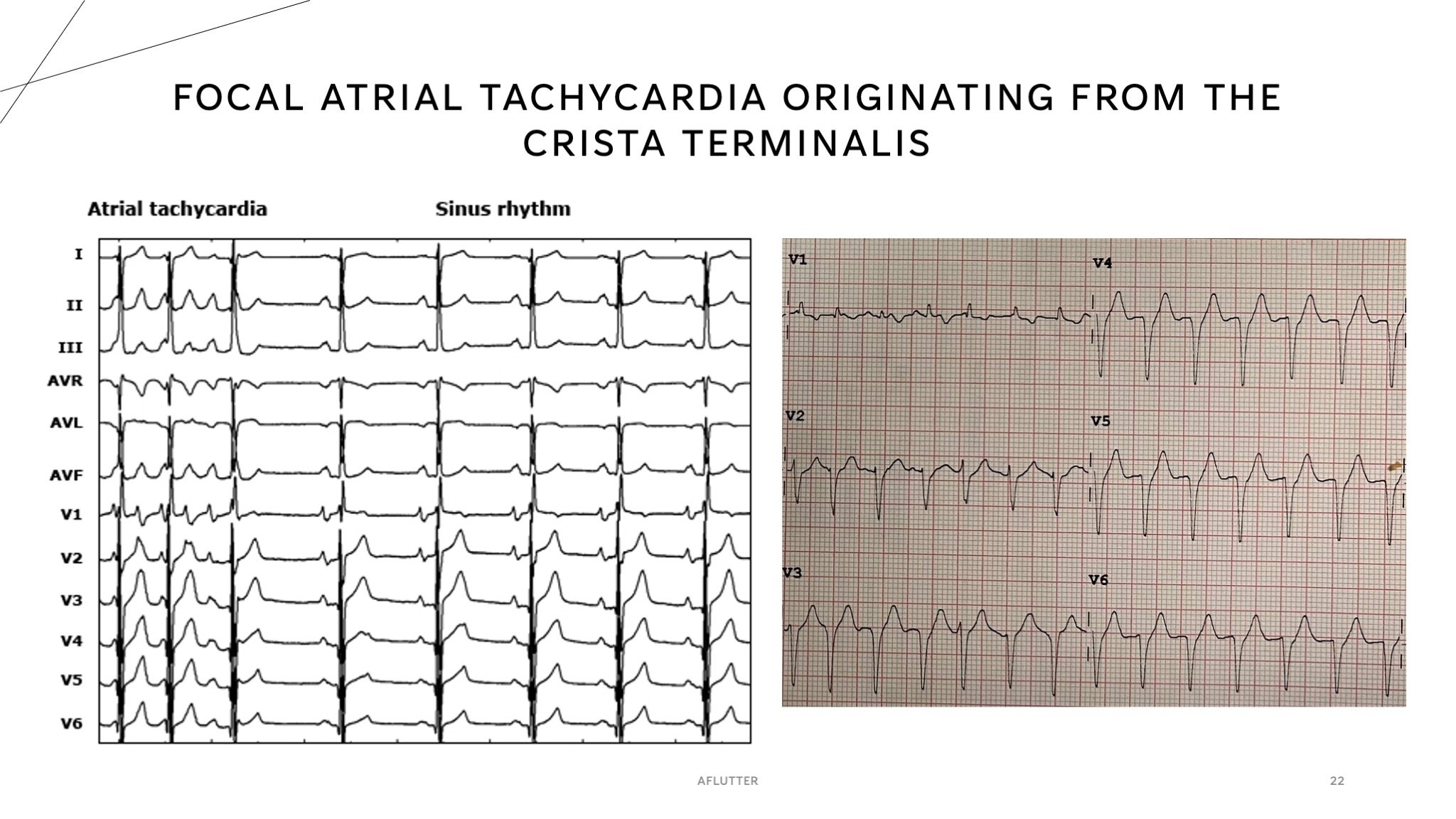
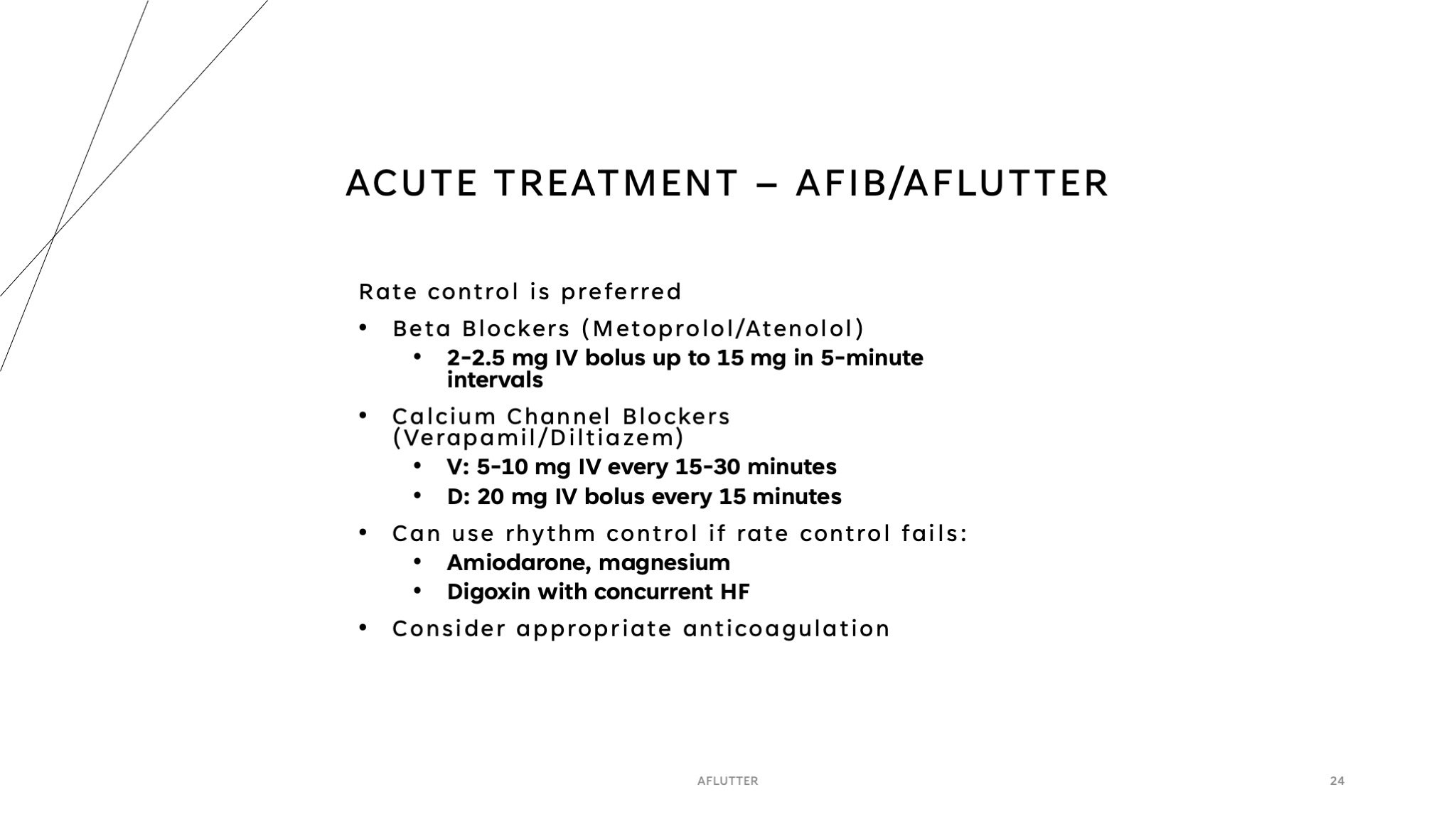
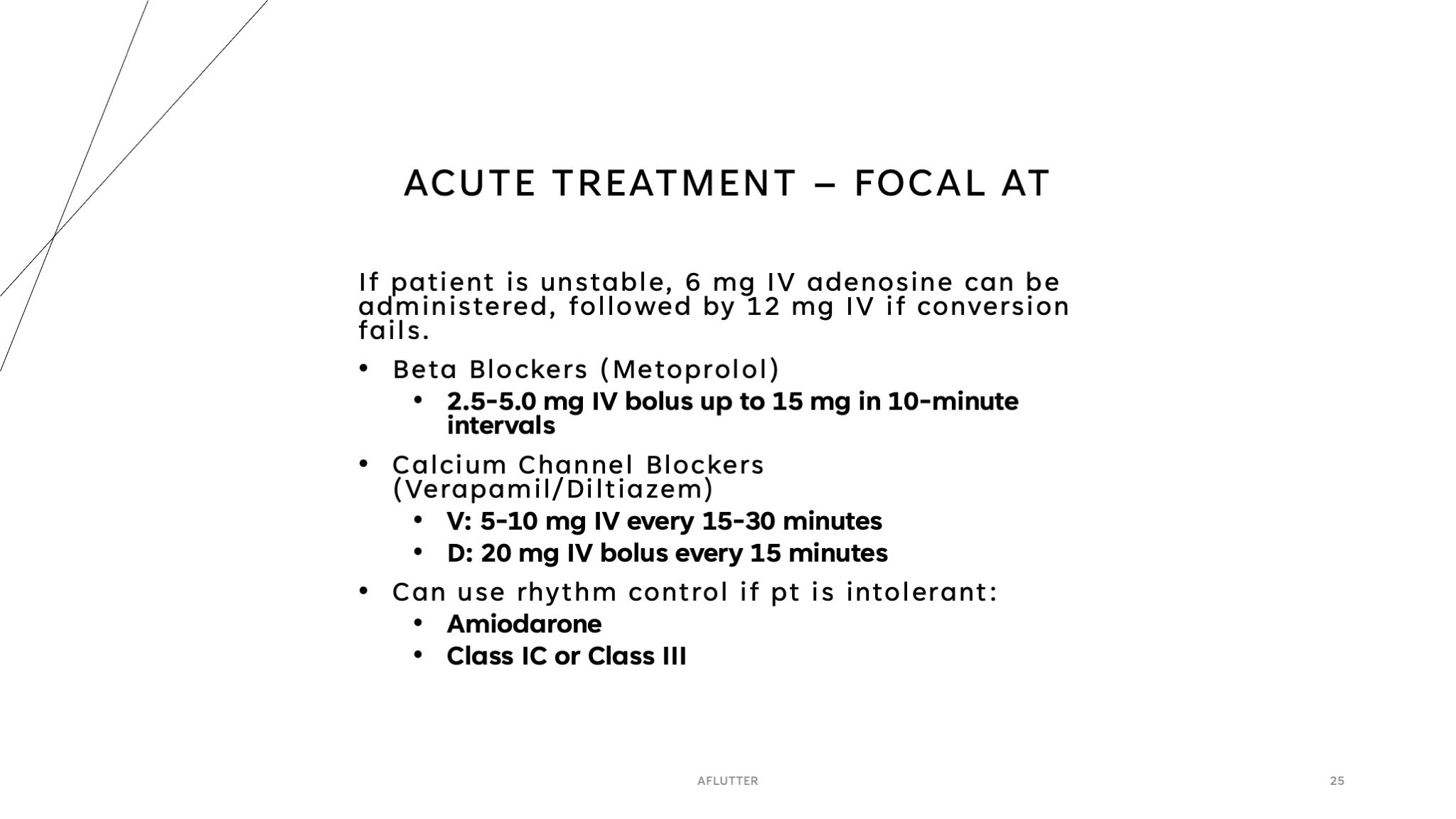
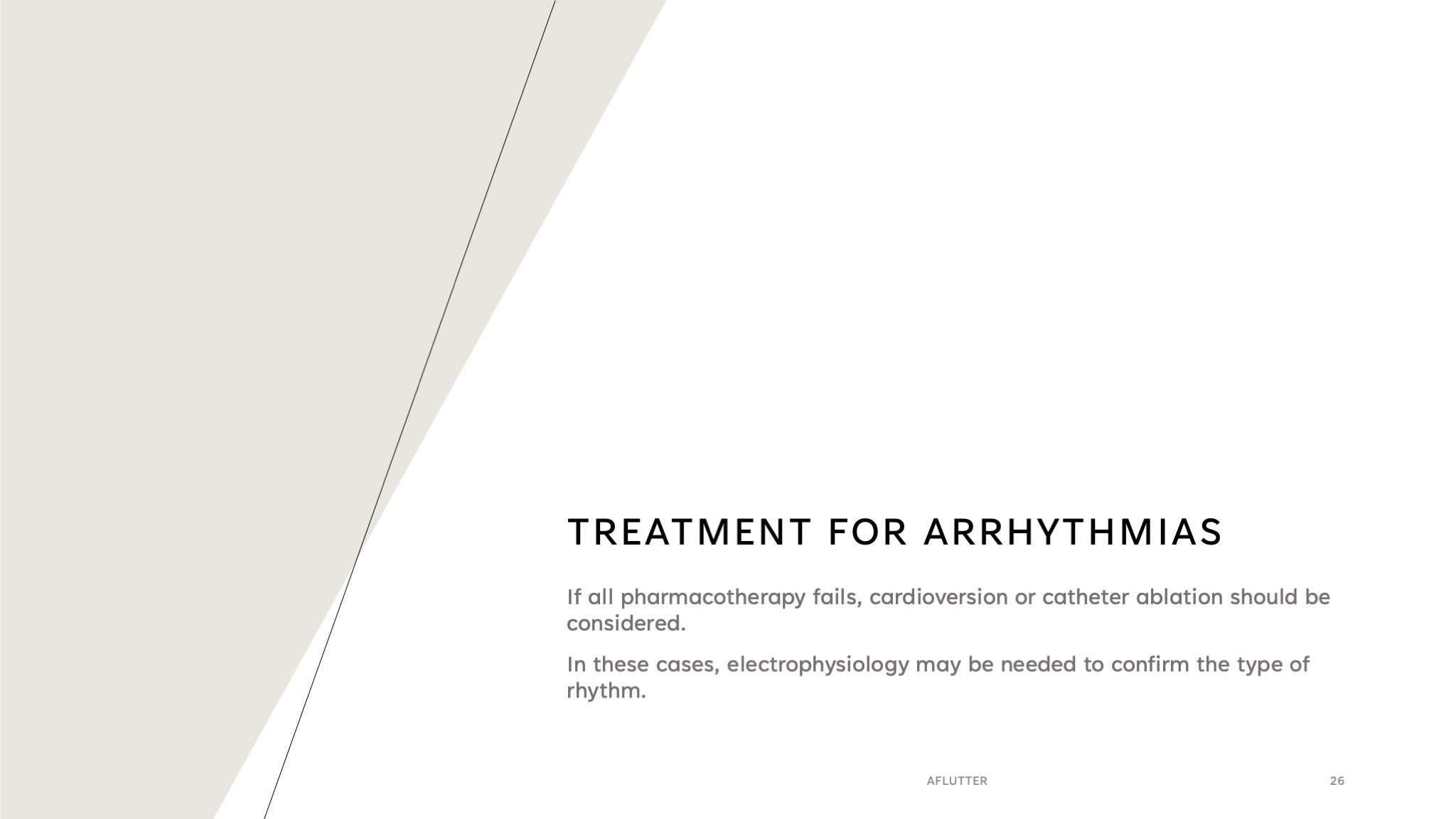
Our final week I did not go to the urgent care clinic, instead we had to go to a didactic session everyday. Monday we had off because of New Years Day. Tuesday we went to internal medicine didactics, Wednesday we had family medicine didactics and a group OSCE using SIM man, Thursday we had internal medicine didactics again, and Friday we had final presentations. I decided to include a few slides from my final presentation below, although this isn’t all of them! Of course I chose something cardiology related lol. It is based off of a patient case with an explanation of the diagnosis pathophysiology and treatment. We had a lot of SOAP notes/H&Ps to do, and you really do start to get the flow of what’s expected. Keep in mind that every resident and physician has their own preferences for how you complete a note, so make sure to always be flexible with how you write yours.
Final Thoughts
In summary, I am SO excited for the next rotations. I feel like I have a solid foundation for moving into the next phase and I’m ready for the challenges that will come along with it. I am staying in Ohio for a full year before moving to RUMC (I think) to finish up my core rotations sometime next November. I definitely want to keep everyone in the loop and I’ll be sure to blog as much as I can throughout the journey so you guys have an idea of what to expect! If there is anything else you guys would like to see or like my to talk about, comment down below and let me know!
Thanks for sticking with me all, and if you are looking for any help, don’t forget to check out the website membership for on-demand lectures and our group sessions or private tutoring for some extra help with pre-clinical content!
Happy Studying <3
